Will Ward at the NSTAR Walk for Boston Children’s Hospital in 2012—his family’s fifth year leading a team to raise funds for the Beggs Laboratory.
This two-part series examines two potential treatment approaches for myotubular myopathy, a genetic disorder that causes muscle weakness from birth.
Sixth-grader William Ward cruises the hallways at school with a thumb-driven power chair and participates in class with the help of a DynaVox speech device. Although born with a rare, muscle-weakening disease called X-linked myotubular myopathy, or MTM, leaving him virtually immobile, he hasn’t given up.
“From the very beginning, Alan connected with our family in a very human way,” says Will’s mother, Erin Ward. “In the scientific community, he’s been the bridge and the connector of researchers around the world. That makes him unique.”
Since the 1990s, Beggs has enrolled more than 500 patients with congenital myopathies from all over the world in genetic studies, seeking causes and potential treatments for congenital myopathies—rare, often fatal diseases that weaken children’s skeletal muscles from birth, often requiring them to breathe on a ventilator and to receive food through a gastrostomy tube. Full story »
Just like Goldilocks wouldn’t eat porridge that was too hot or too cold, blood vessels won't grow properly in tissues that are too stiff or too loose. (Project Gutenberg/Wikimedia Commons)
In the tale Goldilocks and the Three Bears, Goldilocks tries all of the bears’ porridge, chairs and beds, finding that only the little bear’s things were just right. Everything else was a little off for her…too hot or too cold, too hard or too soft and so on.
Similarly, for everything to work as it should in the body, things need to be just right. Blood pressure shouldn’t be too high or too low; organs can’t be too big or too small, etc.
Donald Ingber, MD, PhD, and his lab in Boston Children’s Vascular Biology Program take this “just right” approach when thinking about how organs and tissues are structured. Recently, he and a member of his research staff, Akiko Mammoto, MD, PhD, discovered that by changing the stiffness of the surrounding tissues—not too loose and not too tight— they could keep blood vessels from leaking. Their finding could have real consequences for people with sepsis or other diseases featuring leaky vessels. Full story »
There are a couple of ways by which aspirin might affect cancer. (cpradi/Flickr)
Aspirin does a remarkable number of things in the body, enough that it’s said it would never win approval today from the Food and Drug Administration as an over-the-counter drug.
But among those functions are some that may explain something that doctors have recognized for some time: patients with cancer who have been taking aspirin tend to have better outcomes. Full story »
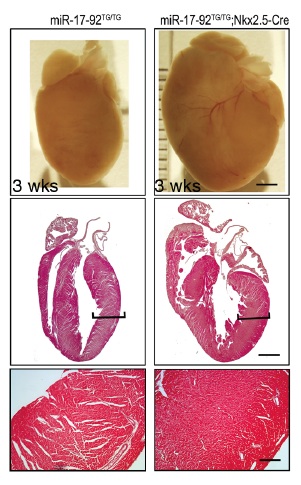
In mice, boosting amounts of a microRNA family called miR-17-92 led to dramatic enlargements of embryonic and postnatal hearts, with thicker ventricle walls.
Challenging accepted wisdom about the heart, Boston Children’s Hospital cardiologist Bernhard Kühn, MD, recently showed that infants, children and adolescents are capable of generating new heart muscle cells, or cardiomyocytes. That work raised the possibility that scientists could stimulate regeneration to repair injured hearts.
Now, we have a potential therapeutic target to accomplish this: a family of microRNAs called miR-17-92 that regulates cardiomyocyte proliferation. In Circulation Research earlier this month, a team led by Kühn’s research colleague Da-Zhi Wang, PhD, demonstrates its potential. Full story »
Leonard Zon (top) and Massachusetts Lt. Governor Timothy Murray in the Stem Cell Program's zebrafish facility. (Courtesy MLSC)
Ed. Note: Leonard Zon, MD, is founder and director of the Boston Children’s Hospital Stem Cell Program, which yesterday was awarded $4 million by the Massachusetts Life Sciences Center to build the Children’s Center for Cell Therapy.
As a hematologist, I see all too many children battling blood disorders that are essentially untreatable. Babies with immune deficiencies living life in a virtual bubble, hospitalized again and again for infections their bodies can’t fight. Children disabled by strokes caused by sickle cell disease, or suffering through sickle cell crises that drug treatments can’t completely prevent. Children whose only recourse is to risk a bone marrow transplant—if a suitably matched donor can even be found.
Over the past 20 years, my lab and that of George Daley, MD, PhD, at Boston Children’s Hospital have worked hard to give these children a one-time, potentially curative option—a treatment that begins with patients’ own cells and doesn’t require finding a match. Full story »
In times past, a pharmaceutical chemist’s main focus was to synthesize novel molecules to treat diseases. Today, an increasingly popular alternative is to re-engineer an existing drug—and continually improve it even after FDA approval. That’s how Robert D’Amato, MD, PhD, developed Pomalyst®, recently approved to treat multiple myeloma and the most potent analog to date of thalidomide.
Thalidomide has its own fascinating history. Originally developed by Chemie Grünenthal GmbH in the 1950s, it was the result of a search for an anti-anxiety drug to compete with Valium, and was approved for use in Europe as a sleep aid and depression treatment. Eventually, doctors found it useful for treating nausea, and started prescribing it off-label to pregnant women with morning sickness.
The results were disastrous. Thalidomide turned out to be a teratogen, causing severe birth defects. Full story »
Recombinant DNA technology might turn bacteria into factories for producing siRNAs. (zoetnet/Flickr)
If you are a scientist and you want to turn off a gene, one option that’s been gaining traction is RNA interference (or RNAi). In this molecular process—first discovered in plants and only 12 years ago detected in mammals—bits of RNA called small interfering RNAs (siRNAs) cancel out a gene’s messenger RNA, effectively muffling that gene.
Labs can order custom-made, chemically synthesized siRNAs for just about any DNA sequence they want to silence. The tricky part is deciding what the right sequence is—especially when that gene is part of a virus, where genes can mutate pretty quickly.
However, a biotechnology approach to producing siRNAs could make it relatively easy for just about any lab that can master recombinant DNA technologies to make a number of siRNAs against multiple sequences within the same target gene: a potential bonus for companies seeking to make drugs that rely on RNAi. Full story »
A technology from a small research institute, originally developed as a safer way to make embryonic-like stem cells, just hooked a very large fish. As The New York Timesreported yesterday, pharma giant AstraZeneca is betting at least $240 million that this technology could be the source of a variety of new drugs—drugs that spur the body itself to make what it needs.
In 2010, the lab of Derrick Rossi at the Immune Disease Institute, which is now the Program in Cellular and Molecular Medicine at Boston Children’s Hospital, reported that they could reprogram ordinary cells into pluripotent stem cells by simply injecting them with messenger RNAs. The mRNAs reprogrammed the cells up to 100 percent more efficiently than other techniques, and did so without becoming part of the cell’s genome, greatly reducing concerns about cancer associated with other methods.
Key to the discovery were the chemical modifications made to the mRNAs so that cells wouldn’t “see” them as viruses and attack them. This video and this article describe the modified mRNA technique, also described in Cell Stem Cell:
If we could immunize infants at birth, far more could be protected from infections.(DFID-UK Dept for International Development)
Right now, immunizations against most infections begin at 2 months of age. But that leaves newborns at risk for infections like rotavirus, whooping cough and pneumococcus during a highly vulnerable time.
In resource-poor countries, this is a serious problem: Many children see a health care provider only at birth, so may miss their chance to be protected. Worldwide, each year, more than 2 million infants under 6 months old die from infections, especially pneumonia. If we could immunize infants at birth, it would be a huge win for global health.
Unfortunately, though, newborns don’t respond to most vaccines. Their immune systems are too immature—which is why few vaccines for newborns exist. Full story »
As the close of American Heart Month draws near, let's take a moment to learn what two teams of scientists are doing to help heart transplant patients keep their new hearts in the long run. (englishsnow/Flickr)
You’re a heart transplant patient. You’ve been on the waiting list for months, maybe years. Now, you’re being wheeled out of the operating room, a donated heart beating in your chest.
You’ve finished one journey, but are only just starting on a new one: keeping your body from rejecting your new heart.
Luckily for you, new methods under development could help tell early on when chronic rejection problems—the kind that arise five or 10 years after your transplant—start to loom. And even better, scientists are homing in on a new way to prevent chronic (and maybe short-term) rejection from happening in the first place. Full story »