
A magnetic needle and thread lets surgeons maneuver in tight spots.
The current method of suturing used in surgery—stitching with a needle and thread—has been around for thousands of years.
Kaifeng Liu, MD, a research fellow at Boston Children’s Hospital, hopes to reimagine this fundamental operating room practice. His workbench is filled with various prototypes of a magnetic needle, a device he hopes will make suturing simpler, faster and more efficient for researchers and clinicians alike.
“Sometimes it is the simplest things in medicine that stay the same over time,” says Liu, whose invention will be featured later this week at Boston Children’s Hospital’s Global Pediatric Innovation Summit + Awards 2014 (October 30-31). Full story »
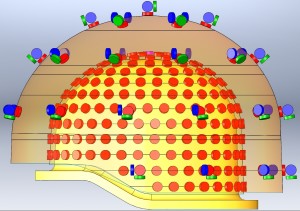
This array of sensors surrounding a baby's head will give researchers and eventually clinicians a high-resolution image of neural activity.
Imagine you’re a clinician or researcher and you want to find the source of a newborn’s seizures. Imagine being able to record, in real time, the neural activity in his brain and to overlay that information directly onto an MRI scan of his brain. When an abnormal electrical discharge triggered a seizure, you’d be able to see exactly where in the brain it originated.
For years, that kind of thinking has been the domain of dreams. Little is known about infant brains, largely because sophisticated neuroimaging technology simply hasn’t been designed with infants in mind. Boston Children’s Hospital’s Ellen Grant, MD, and Yoshio Okada, PhD, are debuting a new magnetoencephalography (MEG) system designed to turn those dreams into reality. Full story »
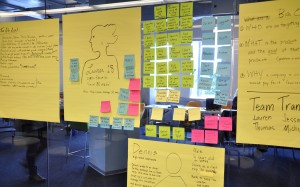
Parents, clinicians, app developers, designers and more had 18 hours to prototype digital healthcare solutions at Hacking Pediatrics, produced by Boston Children’s Hospital and MIT Hacking Medicine. To accompany our earlier post, we created this Storify. Full story »
(Dana Hatic for MedTech Boston)
What are the pain points in pediatrics? There are at least 37: the number of clinicians, parents and others who lined up at the podium last weekend to pitch
problems they hoped to solve at the second annual
Hacking Pediatrics.
The hackathon, produced by Boston Children’s Hospital in collaboration with MIT Hacking Medicine, brought out many common themes: Helping kids with chronic illnesses track their symptoms, take their meds and avoid lots of clinic visits. Helping parents coordinate their children’s care and locate resources. Helping pediatric clinicians make better decisions with the right information at the right time.
Hackathons have a simple formula: Pitch. Mix. Hack. Get Feedback. Iterate. Repeat—as many times as possible. Full story »

Health care institutions, universities and even the U.S. government are helping innovators hone their pitches and get backing.
On ABC’s reality show “
Shark Tank,” a panel of veteran investors listens to business pitches for everything from new dietary supplements to a nail salon for men. After asking tough questions, each shark either backs the venture—sometimes not for the reasons you’d think—or more likely declares, “I’m out.”
It’s a great infotainment formula—even my 10-year-old daughter is a fan—but it’s also a hit beyond the living room. Health care organizations are increasingly borrowing the “Shark Tank” script to get new ideas or to bankroll their own innovations. Boston Children’s Hospital is doing so at our Global Pediatric Innovation Summit + Awards (Oct. 30-31), bringing in “Shark Tank”’s Daymond John to moderate. But we’re certainly not alone. In recent months: Full story »

Start your engines: A fleet of GoBabyGo cars, customized by therapists and parents to give disabled children mobility and help strengthen weak muscles. (Courtesy Cole Galloway)
TEDMED2014 focused on a powerful theme: unlocking imagination in service of health and medicine. Speaker after speaker shared tales of imagination, inspiration and innovation. Here are a few of our favorites:
$100 plastic car stands in for $25,000 power wheelchair
In the first (and likely only) National Institutes of Health-funded shopping spree at Toys R’ Us, Cole Galloway, director of the Pediatric Mobility Lab at the University of Delaware, and crew stocked up on pint-sized riding toys.
Galloway’s quest was to facilitate independence and mobility among disabled children from the age of six months and older and offer a low-tech solution during the five-year wait in the United States for a $25,000 power pediatric wheelchair.
The hackers jerry-rigged the toys with pool noodles, PVC pipe and switches, reconfiguring them as mobile rehabilitation devices to promote functional skills among kids with special needs. Full story »
(gegenart/Shutterstock)
A mouse surrounded by computer screens turns its head when it notices lines moving across one of them, as a camera captures this evidence of visual acuity. A chamber similarly equipped with video cameras tests social interaction between mice. A small swimming pool, with shapes on its walls as navigational cues, lets scientists gauge a mouse’s spatial memory. A pint-sized treadmill, with a tiny camera to watch foot placement, measures gait.
Here in the Neurobehavioral Developmental Core at Boston Children’s Hospital, managed by Nick Andrews, PhD, the well-tended mice also have opportunities to play: “If you have a happy mouse,” says Andrews, “researchers get better, more consistent results.” Full story »
 Naomi Fried, PhD, Chief Innovation Officer at Boston Children’s Hospital, will lead a panel on Innovation Acceleration at Taking on Tomorrow: Global Pediatric Innovation Summit + Awards (October 30-31, Seaport World Trade Center, Boston). Register now!
Naomi Fried, PhD, Chief Innovation Officer at Boston Children’s Hospital, will lead a panel on Innovation Acceleration at Taking on Tomorrow: Global Pediatric Innovation Summit + Awards (October 30-31, Seaport World Trade Center, Boston). Register now!
The word innovation gets thrown around a lot these days by people trying to set their products and ideas apart in the marketplace. But when everything is innovative, is anything really innovative? And if there really are innovative ideas, are they simply flashes of brilliance that can’t be planned for or predicted?
The answer to this last question is “no,” as I see every day at Boston Children’s Hospital, where I lead the Innovation Acceleration Program. The real trick is creating an innovation culture that supports great ideas—but that also supports the not-so-great ideas that teach us almost as much.
So what are the attributes of an innovation culture? Full story »

Fixing a real problem, even a small one, can transform health care.
What can innovators do to work with investors and industry to move an idea toward commercialization? Speakers at the upcoming
Global Pediatric Innovation Summit + Awards, hosted by Boston Children’s Hospital, have some simple advice: Don’t think your innovation has to be sexy.
Health care is plagued by problems that aren’t necessarily sexy or compelling, says Mandira Singh, MBA, of AthenaHealth, who will speak at the Summit’s Mobile & Digital Health panel. More than many other industries, it still depends on outdated technology. For example, it’s the only industry that continues to rely on fax machines. “These are small problems that need to be fixed,” Singh said recently at a Boston Children’s Hospital forum.
Instead of focusing on everyday challenges, innovators often think far out into the future—to where they think health care will be in 10 years. That can be a trap: Full story »
 Technology sometimes unfolds at a slow, measured pace and sometimes at lightning speed. Right now, we are witnessing what is arguably one of the fastest moving fields in biomedical science: a form of genome editing aptly known as CRISPR.
Technology sometimes unfolds at a slow, measured pace and sometimes at lightning speed. Right now, we are witnessing what is arguably one of the fastest moving fields in biomedical science: a form of genome editing aptly known as CRISPR.
CRISPR allows researchers to make very precise—some would say crisp—changes to the genomes of human cells and those of other organisms. You might think of it as a kind of guided missile. Its precision is opening the doors to a wide variety of research and, hopefully, medical applications. Indeed, the possibilities seem to be bound only by scientists’ imaginations.
“For a long time, we have been accumulating new knowledge about which gene mutation causes which disease. But until very recently, we haven’t had the ability to go in and correct those mutations,” explains Feng Zhang, PhD, a core member of the Broad Institute of Harvard and MIT, and one of the method’s pioneers. “CRISPR is one of the tools that is starting to allow us to directly go in and do surgery on the genome and replace the mutations.”
CRISPR stands for Clustered Regularly Interspaced Short Palindromic Repeats. While this name is a bit verbose, it points to the technology’s origins: a set of genetic sequences first discovered in bacteria. Full story »







