 You are what you eat, the saying goes. For some conditions (think cardiovascular disease or type 2 diabetes), there are clear connections between diet, health and illness.
You are what you eat, the saying goes. For some conditions (think cardiovascular disease or type 2 diabetes), there are clear connections between diet, health and illness.
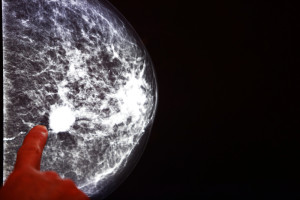
For breast cancer, the picture is less clear. Many epidemiologic and laboratory studies have examined the Western diet (in particular, cholesterol) and its relation to breast cancer, with conflicting results.
“There’s been a raging debate in the field,” says Christine Coticchia, PhD, who works in the laboratory of Boston Children’s Hospital’s Vascular Biology Program director, Marsha Moses, PhD. “The biology of cancer and of cholesterol are so complex, and there are many subsets of breast cancer. In order to find any connections, you have to ask very specific questions.”
Banding together with Keith Solomon, PhD, in Boston Children’s Urology Department, Coticchia and Moses asked whether dietary cholesterol might encourage progression of the most aggressive, so-called “triple-negative” breast tumors. As they report in the American Journal of Pathology, they found a big impact, at least in mice. But it’s too early to say just yet that cutting back on cholesterol will help women avoid breast cancer.
First step: Build a better mouse model
Using a model originally created by the Solomon lab for investigating cholesterol and prostate cancer, the team put laboratory mice on one of four diets:
- low fat/no cholesterol
- high fat/high cholesterol
- low fat/no cholesterol plus the cholesterol-lowering drug ezetimibe (Zetia®), which blocks cholesterol absorption in the gut
- high fat/high cholesterol plus ezetimibe
After four weeks, they injected triple-negative breast cancer cells into the animals’ mammary fat pads. Triple-negative cells, which lack the three major therapeutic breast cancer markers—estrogen, progesterone and HER2 receptors—don’t respond to hormone therapy or the HER2-targeting drug Herceptin®.
The model was geared to be more physiologically relevant than earlier mouse models, which often were geared more toward studying obesity than cancer. “Those mice had cholesterol levels in the thousands, terribly high triglycerides and hyperinsulinemia,” Coticchia points out. “What caused breast cancer in these models? With that many variables, you can’t figure out what the mechanisms are.”
The team controlled for as many variables as possible. For instance, the four diets all had the same number of calories. Throughout the study, there were no differences between the groups in body mass index or triglyceride, insulin or estradiol levels.
The structure of ezetimibe (Wikimedia Commons)
“These mice weren’t obese, they weren’t in metabolic syndrome, they didn’t have dyslipidemia, they weren’t diabetic,” Coticchia states. “We narrowed everything down to one variable: serum cholesterol via dietary intake.”
And why use ezetimibe and not a statin like atorvastatin (Lipitor®) or simvastatin (Zocor®)?
“Statins block the human cholesterol synthesis pathway. They don’t work in mice,” Coticchia explains. And even if they did, she adds, this was a dietary study, and they wanted to block cholesterol absorption (which is how ezetimibe works), not cholesterol production. “If you use a statin, you don’t know if you’re lowering cholesterol because you’re hitting the cholesterol synthesis pathway or because you’re blocking cholesterol in the diet.”
One of these diet groups is not like the others
At the study’s end, tumors in the mice fed the high-cholesterol diet alone averaged about 25 percent larger than those in mice fed the low-cholesterol diet. The difference in tumor size between mice fed the high-cholesterol diet alone versus those also given ezetimibe was even greater: about 50 percent.
However, when Coticchia looked at the amount of cholesterol within the tumors themselves, she found no difference between the diet or drug groups. So even though there was a lot more cholesterol in the blood of the high-cholesterol-diet mice, their tumor cells didn’t take it up.
“The cholesterol was acting on something other than the tumor cells,” Coticchia says. “We suspect it was acting via the vasculature and the tumor’s microenvironment.”
The data bear that theory out. The tumors from the high-cholesterol-diet mice were strikingly more angiogenic—drawing a richer network of blood vessels—than tumors from the low-cholesterol or high-cholesterol + drug groups.
Connecting the dots
Both Moses and Coticchia are quick to caution that their results, while robust, can’t be considered definitive evidence of a link between cholesterol and breast cancer. And they don’t suggest that women should take ezetimibe to reduce breast cancer risk.
“This wasn’t a clinical study,” Coticchia says. “It was a tightly controlled in vivo model intended to answer a very specific research question.”
Moses adds that, from a mechanistic point of view, the study helps connect the dots between cholesterol, angiogenesis and triple-negative tumor growth, and opens up new avenues for further research. “A lot of interesting clinical questions are raised by this study,” she says.
Join us at the Global Pediatric Innovation Summit + Awards 2014 on October 30-31 in Boston. Seats are limited, so register today at www.takingontomorrow.org. Please use the code VECTOR at checkout for a 10% discount.







