 Alexander Rotenberg, MD, PhD, is a pediatric neurologist and epileptologist at Boston Children’s Hospital and director of the hospital’s Neuromodulation Program.
Alexander Rotenberg, MD, PhD, is a pediatric neurologist and epileptologist at Boston Children’s Hospital and director of the hospital’s Neuromodulation Program.
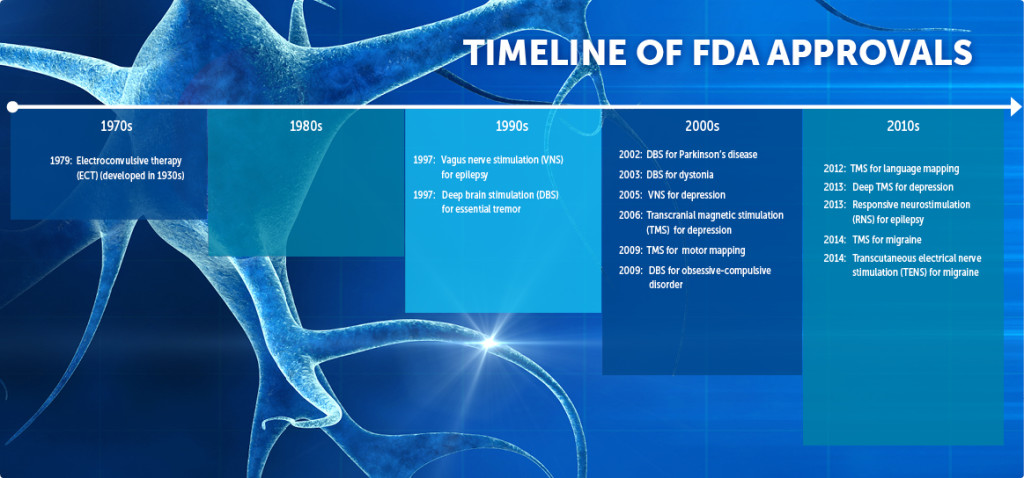
In recent years, electrical devices stimulating the brain or peripheral nerves have emerged as clinical and scientific tools in neurology and psychiatry. In 2014, the Food and Drug Administration has approved three tools at this writing: a device for treatment of epileptic seizures via electrodes implanted beneath the skull; a device for shortening migraine headache via transcranial magnetic stimulation (TMS) of the brain; and a transcutaneous electrical nerve stimulation (TENS) device for migraine prevention. (Click image below for details.)
Stimulating the nervous system to treat neuropsychiatric symptoms is not new. In the first century AD, the Roman physician Scribonius Largus documented treating headaches by applying electric torpedo fish to the head. In the 20th century, electroconvulsive therapy (ECT) was developed to treat drug-resistant depression, vagus nerve stimulation (VNS) to treat drug-resistant epilepsy and deep brain stimulation (DBS) to treat symptoms of Parkinson’s disease.
The 21st century has been witness to an explosion of devices and interest in neuromodulation, a term that describes many brain stimulation techniques that lead to a change in brain function. The growth is driven by three strong trends:
- Medication resistance. There is a growing recognition that a sizeable fraction of common neuropsychiatric disorders, such as major depression, chronic pain and epilepsy, remain resistant to medication. In fact, the proportion of patients whose symptoms persist hasn’t fallen much, despite the improved availability of medications over the past several years. The medical community is, therefore, increasingly looking toward non-pharmacologic treatments.
- Research. Government and industry support for research into aspects of brain biology that relate to brain electrical stimulation is expanding. For instance, the Obama administration’s BRAIN initiative (Brain Research through Advancing Innovative Neurotechnologies) seeks to produce a dynamic picture of brain circuits and proposes allocating $200 million in the President’s 2015 budget.
- Technical advances. Technologies for noninvasive brain stimulation, a family of techniques for measuring and changing brain excitability by applying small electrical currents, are rapidly advancing.
Emerging neuromodulation modalities
TMS, in which small, localized electrical currents are induced into the cortex by a powerful magnetic field, is the most commonly studied noninvasive technique for brain stimulation. It causes little discomfort and (unlike many medications) has a relatively bland side-effect profile. Two TMS devices are presently approved for adults with major depression and another for the treatment of migraine. While there is no FDA approval for therapeutic TMS in children, a TMS device that helps identify motor and speech cortical areas before brain surgery is approved for all ages.
While earlier methods like deep brain stimulation and vagus nerve stimulation require surgery, TMS and tDCS are completely noninvasive. TMS uses a focused magnetic field to induce an electrical field, causing neurons to depolarize and fire. Over time, repeated induced firing seems to change long-term neuronal activity. tDCS applies a weak, direct current to the brain via scalp electrodes, and is thought to cause neurons to change their firing rate.
Still other methods, such as transcranial alternating current stimulation (tACS) and transcranial random noise stimulation (tRNS), are evolving fast and may find a place in patient care. Like TMS and tDCS, these noninvasive brain stimulation protocols have the capacity to change regional brain function with minimal side effects.
While largely preliminary and mostly in adults, the scientific data from clinical trials of noninvasive brain stimulation are encouraging. In rehabilitation, there are promising results showing the capacity for TMS and tDCS to improve motor and language function after stroke. Both techniques also show promise in suppressing pain. In epilepsy, a recent TMS trial shows reduced seizures after treatment, and other trials (including one at Boston Children’s Hospital) are ongoing.
Brain stimulation for children?
As with many medical technologies, adapting brain stimulation to children requires special considerations. Since children are not just small adults, care and caution are required to adapt brain stimulation methods to the biology of a developing central nervous system. Research into the safety and efficacy of neuromodulation in pediatrics is ongoing in many medical centers, including Boston Children’s, where the Department of Neurology recently launched a Neuromodulation Program.
The recent scientific advances in noninvasive brain stimulation are good reason for cautious optimism. Like most electronics, neuromodulation tools get better and cheaper each year, and this translates to better access for patients and physicians. The Boston Children’s Neuromodulation Program will offer these tools for children and adolescents with neuropsychiatric disorders such as autism, depression, intractable pain and epilepsy, and will include a research arm to evaluate whether they improve care.
We hope this will be a step toward increasing the number of treatment options available to children with drug-resistant neuropsychiatric symptoms. Stay tuned.
To learn more about supporting work in the Rotenberg lab, contact [email protected].







