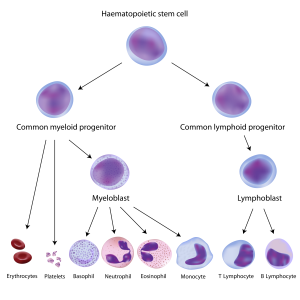
Blood-forming hematopoietic stem cells (top) give rise to all blood and immune cell types. In children with SCID, the steps leading to immune cells are broken.
In the world of fatal congenital immunodeficiency diseases, good news is always welcome, because most patients die before their first birthday if not treated. Babies with severe combined immunodeficiency disease, aka SCID or the “bubble boy disease,” now have more hope for survival thanks to two pieces of good news.
Transplants are looking up
First came a July paper in the New England Journal of Medicine (NEJM) by the Primary Immune Deficiency Treatment Consortium. This North American collaborative analyzed a decade’s worth of outcomes of hematopoietic stem cell transplant (HSCT), currently the only standard treatment option for SCID that has a chance of providing a permanent cure.
The review looked at how a range of factors affected the five-year survival of 240 patients, providing important insights into what works and what doesn’t when transplanting hematopoietic stem cells from another person into patients with SCID, such as:
- Transplants work. Overall, 74 percent of infants survived at least five years.
- Early diagnosis and treatment matter. Ninety-four percent of infants who received a transplant before turning 3 ½ months old were alive at 5 years.
- Infections have a big impact. Infants older than 3 ½ months still fared well as long as they didn’t have an active infection when they were treated: 90 percent were alive at 5 years. But only 50 percent of older infants with an infection at the time of transplant survived to the five-year mark. That number was even lower—39 percent—if an infant had an infection AND did not have a matched sibling donor.
“Previously, we didn’t know which was more important, age or infection,” says Sung-Yun Pai, MD, a pediatric hematologist-oncologist with Dana-Farber/Boston Children’s Cancer and Blood Disorders Center and the study’s lead author. “These data say clearly that infection status has a large impact on survival.”
Pai adds that the age and infection data bolster the case for expanding newborn screening for SCID. Twenty-one states and the District of Columbia—all told, home to about two-thirds of all babies born in the United States—screen newborns for SCID. Nine more states should start by year’s end.
“Time is not the ally of children with SCID,” says Boston Children’s Hospital’s Luigi Notarangelo, MD, one of the study’s senior authors and one of many who lobbied successfully to establish SCID newborn screening in Massachusetts in 2009. “Because these infants do not have a functional immune system, the longer the wait before a transplant the greater the risk they will contract a potentially devastating infection.”
Safety and success for gene therapy
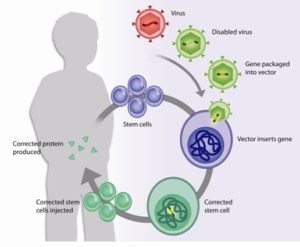
Gene therapy in action. Doctors take hematopoietic stem cells from the patient, use a viral vector to insert a gene, and give the cells back.
Now for the second piece of good news. For some infants with SCID, an HSCT isn’t an option. It may be that there’s no acceptable donor available, or that the child has other risk factors that make a transplant too dangerous.
In a second NEJM paper published a couple of weeks ago, Pai, Dana-Farber/Boston Children’s David Williams, MD, and their collaborators in the Trans-Atlantic Gene Therapy Consortium (TAGTC) revealed promising initial results from a clinical trial of gene therapy in boys with a subtype of SCID called X-linked SCID (or SCID-X1).
The protocol used a genetically engineered virus to deliver a working copy of the IL2RG gene (which is broken in boys with SCID-X1) into nine boys with the disorder (including Agustín Cáceres, who traveled from Argentina to be the first boy treated in the trial in the U.S.).Unlike HSCT, where the cells are donated from another individual, each boy served as his own donor.
One to more than three years post-treatment, eight of the nine boys are alive and well, with functioning immune systems and no sign of SCID-associated infections (one of the eight, however, ended up needing a cord-blood stem cell transplant). The boy who died succumbed to an infection before his genetically corrected cells had enough time to fully restore his immune system.
At the trial’s heart was a modified virus vehicle—called a viral vector—designed to more safely shuttle the gene into the patient’s cells. In a prior SCID-X1 gene therapy trial in Europe—the first to show that gene therapy could cure a human disease—the vector activated cancer-causing genes. As a result, a quarter of patients developed leukemia three to five years after gene therapy. The goal with this trial’s improved vector, called a self-inactivating gammaretroviral vector, was to reduce or eliminate the risk of leukemia down the road.
The SCID team at Boston Children's and Dana-Farber/Boston Children's (l-r): Luigi Notarangelo, MD; David Williams, MD; Sung-Yun Pai, MD.
The vector redesign seems to have paid off. While the TAGTC team will continue to monitor each patient for 15 years for signs of leukemia, genetic and molecular studies show no obvious activation of any cancer-causing genes, including those implicated in the last trial.
“The efficacy data from our study are clear: The vector does work to correct the disease,” says Williams, who is a leader of Dana-Farber/Boston Children’s, chief of the Division of Hematology/Oncology and director of clinical and translational research at Boston Children’s Hospital. “And by a surrogate endpoint, we have improved the treatment’s safety, although it’s too early to say that we’ve completely eliminated the long-term risk of leukemia.”
If you like success stories like this, you’ll love our Global Pediatric Innovation Summit + Awards 2014, taking place on October 30-31 in Boston. The summit is sold out, but keep checking www.takingontomorrow.org or follow the hashtag #pedinno14 on Twitter to stay on top of the action.






