 Despite recent national pediatric guidelines recommending identification and treatment of children with familial hypercholesterolemia, the use of lipid-lowering treatment has been flat over the past decade in real-world pediatric practice, finds a large multicenter study.
Despite recent national pediatric guidelines recommending identification and treatment of children with familial hypercholesterolemia, the use of lipid-lowering treatment has been flat over the past decade in real-world pediatric practice, finds a large multicenter study.
Justin Zachariah, MD, MPH, a pediatric cardiologist at Boston Children’s Hospital, presented the findings this week at the 2013 American Heart Association (AHA) Scientific Sessions. He believes they dispel some critiques of the recent guidelines, particularly concerns that more screening would result in overmedicating the pediatric population.
Extending beyond 2008 recommendations from the American Academy of Pediatrics, the 2011 National Heart, Lung and Blood Institute’s pediatric guidelines call for universal lipid screening and medical treatment for children at highest risk for early cardiovascular disease. One such high-risk condition is familial hypercholesterolemia, a genetic disorder characterized by high blood cholesterol levels, specifically very high levels of low-density lipoprotein (LDL, or “bad” cholesterol) and early coronary events.
“If a child has a copy of the disease-causing gene from both parents, he or she will often have a heart attack by age 20,” Zachariah says. “It manifests itself with an LDL cholesterol in the high hundreds to the 1,000 range, whereas normal is below 130. If you have one bad copy of the gene, your LDL will generally range from the 200s to 400s.”
Decreased lipid testing, flat lipid-lowering treatment
The mutation is relatively uncommon—about one patient in 1 million has two copies and one patient in 500 has single copy (by comparison, Down syndrome occurs in approximately 1 in every 1,000 births). But the effect is potent: Men with one bad copy of the gene have a 50 percent chance of having a heart attack before age 50, and women 20 to 25 percent—which is 20 to 100 times higher than the general population, Zachariah says.
“Because in most patients this genetic disorder isn’t externally recognizable, the 2011 guidelines suggested that clinicians begin screening for this disease with blood tests in all kids,” Zachariah explains.
“We found that the number of children on lipid-lowering medications was quite low,” says Zachariah, “And, based on previous literature, inappropriately low.”
Yet, he and his colleagues found that fewer children were checked for lipid problems in 2012 as compared with 2002. Their study queried the Cardiovascular Research Network, which is funded by the National Institutes of Health, yielding a pediatric outpatient population of 228,783 children 2 to 20 years old. Seeking a heterogeneous study population, they assessed databases from Texas, Michigan, Wisconsin and Hawaii, including at-risk minority populations.
Between 2002 and 2012, the proportion of children n being checked for lipid problems decreased from 17 percent to 12 percent. At the same time, more of the children who were checked had cholesterol problems related to obesity. Yet, as the researchers point out, a large number of children with high cholesterol, including those with genetic cholesterol disease, are not obese.
New cholesterol prescriptions fell from 0.07 percent to 0.02 percent, keeping the proportion on medicine in each year about 0.08 percent, less than half the expected prevalence of 0.2 percent for familial hypercholesterolemia:
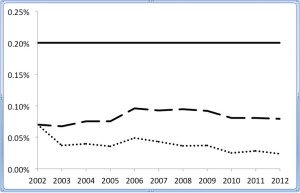
Cholesterol medicine use in 2- to 20-year-old patients, 2002-2012. The dotted line denotes the percentage with a new cholesterol-lowering prescription each year, the dashed line represents those on treatment and the solid line defines the expected proportion with genetic familial hypercholesterolemia.
“We found that the number of children on lipid-lowering medications was quite low,” says Zachariah, “And, based on previous literature, inappropriately low.”
Currently, the researchers are expanding their study to include more health care facilities across the U.S. that are also part of the network, in hopes of capturing data on more than 500,000 children in total.
The new guidelines have received a fair amount of criticism, but continue to be defended on the basis of averting a catastrophic event with a vulnerable—albeit small—population.
Cholesterol medicine use in 2- to 20-year-old patients, 2002-2012. The dotted line denotes the proportion with a new cholesterol medicine prescription each year, the dashed line represents the proportion on treatment and the solid line defines the expected proportion with genetic familial hypercholesterolemia.







