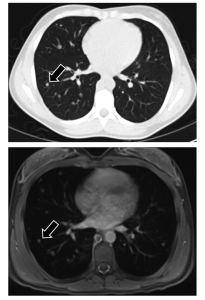
With the latest technologies and techniques, MRI (bottom) is in many cases just as good as, if not better than, CT (top) when taking images of a child's chest. (Courtesy Edward Y. Lee, MD, MPH)
Magnetic resonance imaging, or MRI, can produce stunningly detailed images of the body’s tissues and structures. Historically, however, the chest—and in particular, the lungs and airway—has proven challenging for radiologists to clearly visualize through MR images.
Why is that? Unlike most other solid organs, the lung and trachea aren’t really solid. The air spaces within them do not absorb the magnetic fields or produce the radio signals needed to generate high-quality diagnostic images. Also, they are in constant motion—we have to breathe, after all.
For these reasons, radiologists have long relied on x-rays and computed tomography (CT) scans to take pictures of the lungs. Both can produce very good, highly detailed diagnostic images, but both also come with risks related to their reliance on ionizing radiation.
The lung MRI’s time may now have come. In a review paper in Radiologic Clinics of North America (RCNA), an international team of radiologists led by Simon Warfield, PhD, and Edward Y. Lee, MD, MPH, of Boston Children’s Department of Radiology outlines several recent advances that have made MRI a more viable—radiation-free—alternative for diagnostic imaging of children’s lungs and airway.
“MRI has been around for a long time now,” says Lee, chief of thoracic imaging and director of MRI at Boston Children’s. “With high-resolution 3T scanners, advanced imaging techniques and improved methods of pediatric patient preparation now available, it’s quite possible to image the lung and airway with MRI for diagnostics purposes.”
In the RCNA paper, Lee, Warfield and their co-authors note that improvements in imaging protocols—such as 3-plane T1-weighted gradient recalled echo (GRE) localizer; coronal T2-weighted single-shot half Fourier turbo spin echo; and axial T1-weighted 3D GRE volumetric interpolated breath-hold—and the use of improved contrast agents have all contributed to making MRI a viable option for chest imaging in children. Having patients breathe hyperpolarized xenon or helium gas or 100 percent oxygen also can help improve images of lung or airway ventilation, down to the alveolar level.
The mix of methods that a radiologist chooses would depend on the purpose for the images, such as evaluation of chronic lung diseases like cystic fibrosis, structural defects in the lungs or airway or lung infections.

(l-r) Reid Nichols, Diane Biagiotti, RT, Simon Warfield, PhD, Edward Y. Lee, MD, MPH, and Valerie Dinan, RN, of Boston Children's MRI team.
Patient preparation and training in breathing control have also helped improve image quality. A patient’s ability to hold his or her breath for short periods of time is crucial to chest MRI, lest the scan come out with too many motion artifacts for diagnostic use. I can hold my breath for about a minute, but my 9-year-old son can only do it for about 15 seconds; same for my 5-year-old.
“Children can have a hard time with breathing instructions for MRI in part because they can be quite complex,” Lee explains. “But by properly training young children, 4 or older, before imaging, we can often obtain high-quality MR images. Infants and young children under 4 years old may still require sedation and breath-hold techniques, however.”
Lee adds that MRI image-capture sequences like free-breathing Propeller (BLADE with navigator) can help technologists take images in children who are unable to follow breathing instructions. Additionally, with efforts to make the environment in the MRI suite as child-friendly as possible and offer appropriate distractions, most children over the age of 4 can undergo an MRI without sedation.
In a separate prospective study published in the June’s American Journal of Roentgenology, Lee and colleagues directly compared MRI and CT head-to-head—the first time anyone had done so in both pediatric and adult patients—concluding that:
“Use of MRI with fast-imaging sequences without contrast administration as a first-line, cross-sectional imaging study in lieu of contrast-enhanced [multidetector] CT has the potential to benefit [pediatric patients] owing to reduced radiation exposure and IV contrast administration.”
“MRI has been in clinical use since the 1970s and can produce images that are beautiful to behold and incredible in their capabilities,” says Thomas Martin, MD, a pulmonologist and cystic fibrosis specialist at Boston Children’s who was not involved in Lee and Warfield’s study. “This paper illustrates the range of current clinical and potential research uses of MRI for pediatric chest problems, such as congenital malformations, malignancies and diseases, primarily involving the airways or lung tissue.
“Drs. Lee and Warfield and their team make a strong case that MRI can now be considered equivalent or superior to CT for detecting many abnormalities in pulmonary tissues, and it can be performed successfully for most indications in children of all ages,” he adds.
Henry Dorkin, MD, who directs the Cystic Fibrosis Center at Boston Children’s, adds “Between MRI and CT, we have an incredible suite of imaging technologies available now for imaging [pediatric lungs],” he says. “But what’s most important is making sure we use the right technology to answer the question. Close communication between physicians, radiologists and technicians is key to making sure that we all do what’s best for the patient in front of us.”
Learn more about MRI at Boston Children’s Hospital on the Department of Radiology website.






